Laparoscopic bowel graspers, otherwise known as bowel forceps, are a form of grasping instrument designed to safely manipulate delicate abdominal tissue during laparoscopic procedures. One of their main functions is to facilitate adequate access to the surgical site by holding bowel tissue clear of the operating field.
In its simplest form, a trocar is a pen-shaped instrument with a sharp triangular point at one end, typically used inside a hollow tube, known as a cannula or sleeve, to create an opening into the body through which the sleeve may be introduced, to provide an access port during surgery. The tip design of trocar instrumentation is something that is constantly evolving. The materials, edge design and transparency are factors that may facilitate placement inside the abdominal or thoracic cavity.
Needle drivers, or needle holders, are used to grasp and manipulate needles to enable free-hand suturing of wounds or surgical incisions within the body during laparoscopic procedures. Surgical needle drivers have been in widespread use for little over a century. Prior to this, needles were large enough to be manipulated by hand, and any instruments that were developed to assist with suturing often had more in common with the tools of tailors, sail-makers or leatherworkers than with the surgical instruments of today.
Analog medical cameras have been available since the mid-1970s, but were initially very heavy and could not be disinfected, limiting their usefulness in surgical applications. A major breakthrough occurred in 1982, when the first solid-state medical camera was introduced. Based around a silicon chip called a charge-coupled device (CCD), these digital cameras were lightweight, sterilisable, and offered improved color stability. CCDs are now commonly found in many consumer products including digital cameras and webcams. They consist of a silicon chip covered in image sensors, known as pixels, which convert incoming light energy from a visual scene into a digital signal that can be stored, processed or transmitted with greater efficiency and reliability than its analog equivalent.
Today, a typical laparoscopy system consists of four main components: One or more digital cameras, a light source, a monitor and the scope itself.
The esophagus is a relatively simple organ but it does have several locations where problems are more likely. The most problematic area is at the bottom (technically, in the lower thoracic section) where the esophagus connects with the stomach – the gastroesophageal junction. At the junction is the lower gastroesophageal sphincter, a hole into the stomach controlled by a set of muscles that opens to allow food to enter the stomach, and closes to prevent stomach acid from entering the esophagus. When this sphincter is not functioning properly, especially as a chronic long-term condition, there are many potential problems, some of which may lead to cancer.
Adrenalectomy is the surgical removal of all or part of an adrenal gland. The most common indicator for adrenalectomy is the presence of hormone-producing adrenal tumors. Prognosis is dependent upon individual medical history.
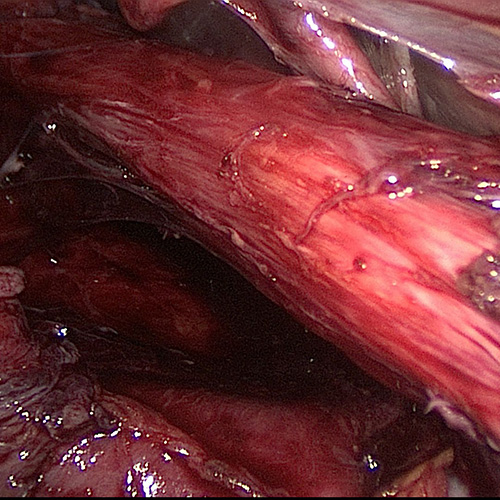
The spleen is located in the top left portion of your abdomen. Operations on the spleen require a very careful dissection around a portion of the stomach, a portion of the pancreas, a portion of the colon as well as the edge of one of the kidneys. A large portion of the operation involves a dissection just above the pancreas. This image demonstrates the first stages of identifying the artery and the vein to the spleen. The blue vessel between the jaws of the dissector is the splenic vein, the yellow tan tissue at the bottom left of the picture is the pancreas.
Diagnosis of a condition suggesting a pancreatectomy can be complicated. It starts with the patient condition, which usually involves considerable pain, weight loss or jaundice (yellow colored skin). These are also symptoms of other diseases, which is typical of most pancreas conditions, making them difficult to diagnose in the early stages. A major consideration will be the overall health of the patient, including risk factors such as obesity, tobacco smoking, alcoholism, diabetes, cardiovascular conditions, family history, age and lifestyle (especially diet).
The main symptom of GERD in adults is frequent heartburn, also called acid indigestion; burning-type pain in the lower part of the mid-chest, behind the breast bone, and in the mid-abdomen. Surgery is an option when medicine and lifestyle changes do not help to manage GERD symptoms. Surgery may also be a reasonable alternative to a lifetime of drugs and discomfort. Fundoplication is the standard surgical treatment for GERD. Usually a specific type of this procedure, called Nissen fundoplication, is performed. During the Nissen fundoplication, the upper part of the stomach is wrapped around the LES to strengthen the sphincter, prevent acid reflux, and repair a hiatal hernia.