

Morbid obesity marks the threshold where diet and exercise no longer work for weight-control. For the right individual, bariatric surgery may be the best option to regain control of their health.
Obesity is a worldwide problem as one in eight people in the world are living with obesity. Obesity affects almost every body system including the heart, lungs, and the hormonal system that balances sugar. As increasing body weight makes exercise more difficult, losing weight becomes more difficult. Ironically the more you typically eat, the hungrier you become between meals, and the harder it is to feel full. Obesity also negatively affects the metabolism of this increase in calories consumed. Obesity may start to spiral and become a self-repeating cycle of negative reinforcement.
Morbid Obesity may sometimes be best treated by breaking this cycle with surgery. Bariatric and Metabolic Surgery is a broad term for surgical procedures that include the gastric bypass and gastric sleeve.
When should I consider Bariatric Surgery instead of Medications?
Bariatric surgery and GLP-1/GIP medications (such as Ozempic, Wegovy, tirzepatide, Mounjaro, and Zepbound) stand as the most powerful tools for treating severe obesity. These are not interchangeable options, they operate through fundamentally different mechanisms, carry distinct risks and benefits, and are best suited to different patients.
Bariatric surgery permanently reshapes gut anatomy, altering hormone signaling (GLP-1, PYY, ghrelin) in a way that endures without ongoing treatment. It delivers superior magnitude and durability of weight loss, especially in severe obesity (BMI ≥50), and more reliably resolves comorbidities like sleep apnea, joint disease, and other mechanical complications of obesity.
For patients who require >25–30% sustained weight loss and seek true diabetes remission without lifelong injections, bariatric surgery remains the gold standard.
A personal look at obesity and its problems

How is Morbid Obesity Defined?
Morbid obesity is defined as a body mass index (BMI) greater than 40 kg/m² and is classified as Class III Obesity. Although this calculation depends upon both an individual's height and weight, persons who are approximately 100 pounds over their ideal body weight are likely to be morbidly obese. Depending on the study, estimates for obesity in America may suggest that up to 35% of adults (or one in every three) suffers obesity and that from between 3–7% of the adult US population currently suffers from morbid obesity.
Several life-threatening complications such as diabetes, high blood pressure and coronary artery disease are associated with this condition. Medical weight reduction practices often do not yield good results in these situations. Surgical intervention may be indicated to stop weight gain, achieve weight loss and reverse some of the obesity-related medical conditions described above.
Metabolic surgery, including gastric bypass and the laparoscopic gastric sleeve, are surgical procedures whose utility in combating morbid obesity are recognized by both medical and surgical specialists. Patients who have a BMI greater than 35 or those with a BMI of 30 or more who are also suffering from life-threatening illnesses curable with weight loss are considered as possible candidates for bariatric surgery.
The decision to proceed with surgery always represents a comparison between risks and benefits, as any surgical procedure involves some risk. Generally accepted criteria for proceeding with this type of surgery include that an individual have been obese for at least two years, be between the ages of 18 and 65 years and have no medical or psychiatric contraindications to undergoing surgery. Many surgeons will consider offering surgery both for younger and older patients than suggested above.
Obesity limits daily function

The disease of morbid obesity interferes with basic physical functions such as breathing or walking. Long-term implications of the disease include shorter life expectancy, serious health consequences in the form of weight-related conditions such as type 2 diabetes and heart disease, and a lower quality of life with fewer economic and social opportunities.
What are Obesity Related Co-morbid Conditions?
Bariatric surgery may improve some pre-existing health conditions. The presence of obesity increases the risk of a number of medical conditions, including cancer. A co-morbid condition is a health condition related to a primary disease such as obesity.
Type II diabetes, heart disease and high blood pressure, high cholesterol, obstructive sleep apnea, acid-reflux, cancer, depression, osteoarthritis and abnormal menses are all examples of obesity related co-morbid conditions. Bariatric surgery can also help women become pregnant and have healthier pregnancies. Weight-loss and dietary change can cure certain elements of PCOS and often times irregular menses begin to normalize and fertility improves.
Restriction, Malabsorption and Hormonal Change
There are several different bariatric surgery procedures, but the two general ways in which they work are restriction and malabsorption:
Restriction limits the amount of food you can eat. The surgically-created, smaller stomach pouch that is created in both the gastric bypass and the gastric sleeve, restricts the amount of food that can be eaten at one time and also ensures that the patient feels satisfied with less food.
Malabsorption limits the number of calories and nutrients your body can absorb. During malabsorptive procedures, the surgeon reroutes the small intestine so that fewer calories and nutrients are absorbed.
The Gastric Bypass

The laparoscopic gastric bypass and the laparoscopic gastric sleeve have many similarities and differences. The skin incisions used to perform the laparoscopic operations are so similar that a doctor can often not tell which operation you have had just by looking at the incisions on your skin.
Patients who undergo bariatric surgery, either laparoscopic gastric bypass or the laparoscopic gastric sleeve, experience significant weight loss after surgery. Both operations decrease the size of the functional stomach, causing an individual to feel full faster. This lowers the amount of food that one consumes and can significantly lower the number of calories consumed.
The Gastric Sleeve
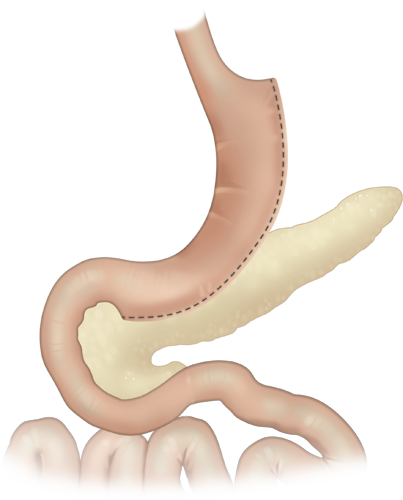
There are many important differences concerning how your intestinal system is changed on the inside. Even though the cuts on the outside of the skin are small, both operations involve cutting the stomach permanently and are associated with real surgical risk. Both operations seem to have positive temporary hormonal effects on satiety and hunger. These positive effects only last about one year at which point you will have hopefully come close to a new healthier weight; you will need to rely on lifestyle modification to maintain your long-term weight loss.
Who Succeeds with Bariatric Surgery?
Long-term success after bariatric surgery is achieved by those who find internal motivation for success and understand that bariatric surgery is a finite tool that can help them achieve their weight-loss goals.
Bariatric surgery can help patients effectively and permanently improve their health. Bariatric surgery restricts the amount of food patients can eat and, depending on the procedure, the number of calories and nutrients the body can absorb. The patients that succeed typically use the surgery as a tool to help them realize and change their previous destructive cycle of bad food behavior.
Dr. Belsley typically recommends a minimum of a 3 month program performed with your primary care doctor even if your insurance carrier does not have a time requirement. Other criteria include an organized set of measurements that has varied over time with one of them representing an estimate of about 100 pounds over your ideal body weight. Ideally you will be at a time and place in your life when you want to improve.
Bariatric surgery should not be considered until you and your doctors have explored dietary weight-loss and lifestyle change. Bariatric surgery is not cosmetic surgery and does not involve the removal of adipose tissue (fat) by suction or surgical removal. You must understand the benefits and risks and commit to long-term lifestyle changes, including diet and exercise, which are key to the success of bariatric surgery.










